There are many of lessons we can learn from Accountable Care Organisations when thinking about ICS contracts says Paul Taylor.
A recent publication “Risk and Reward Sharing for NHS Integrated Care Systems” published by the Midlands and Lancashire CSU’s Strategy Unit gives some interesting insights for fledgling ICS financial arrangements. Whilst there are many differences between American ACO and English ICS arrangements, both are trying to achieve similar financial objectives – managing the rising costs of healthcare.
The Strategy Unit have reviewed the well established risk and reward arrangements in the USA and have identified some interesting learning points for us. The Centers for Medicare and Medicaid Services (CMS) has created a formal approach to risk and reward sharing for US Accountable Care Organisations; the Shared Savings Program. Their approach is both comprehensive and well established.
There are 3 tiers of risk sharing that ACOs can adopt – Track 1, where there is no down-side risk for the ACO but limited upside potential, and Tracks 2 and 3 which give more upside and downside risk. ACOs tend to start on Track 1 and then progress to Track 2 and 3 when they get established. Interestingly the vast majority (90%) of ACOs continue to choose to be on Track 1 showing a limited appetite for risk in the US, where the ACOs tend to be significantly smaller than the intended size of English ICS.
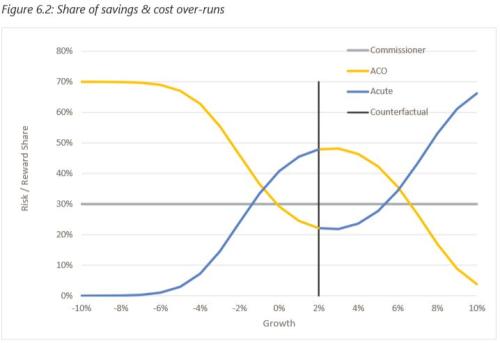
The paper also discusses the part played by the calculation of the counterfactual in determining how the risk and reward mechanism is framed, and how it might be calculated. (My favourite example to help understand the counterfactual concept is “if I hadn’t have run I would have missed the bus”!)
The paper also shows how savings and risks in the US are capped dependent upon which Track you are on. Random variation is also accounted for by not allowing savings or costs to be earned or paid within a narrow margin.
Finally, the paper shows us that the calculation of counterfactuals and risk sharing agreements in the States are complex undertakings and that simplistic approaches in England are likely to lead to unwitting consequences.
There’s lots of food for thought in this publication for anyone working in an existing ICS on financial issues, or anywhere in the NHS where the National Tariff (or Payments by Results) approach is seen to be passé. The simple adoption of a block contract is unlikely to provide the correct incentives for both commissioner and provider. The lessons from the States is that it’s complicated stuff, and that organisations are being very careful before stepping into expansive risk and reward arrangements.
Paul Taylor, Provex Solutions Limited
June 2018