Discharged without a diagnosis
In 2023/24, one million people who were admitted to an NHS hospital in an emergency, were later discharged without a diagnosis. This long-read examines what this means for patients and providers.

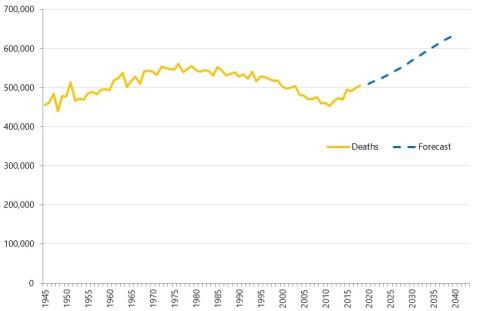
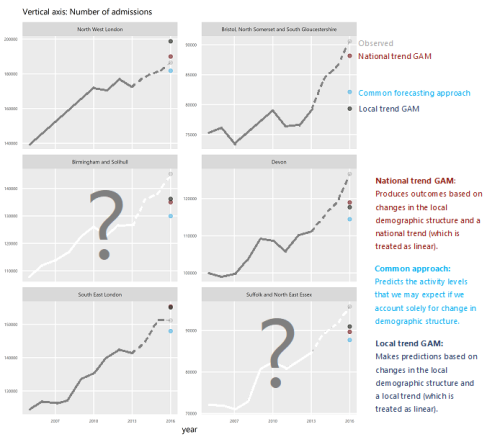
What explains the recent growth in hospital activity?
In this long read, Fraser Battye describes our analysis of what has driven the growth in hospital activity.

Mending smarter, not harder: Changing fracture care for children
The report demonstrates there is significant variation between trusts in England in how paediatric fractures are managed. Widespread adoption of less interventional approaches to paediatric fracture management could result in significant savings in hospital activity, particularly reduced follow-up appointments for uncomplicated fractures.

‘Internal Consultancy’: INSIGHTS from evidence and experience
In this blog, our Head of Policy, Fraser Battye, shares his reflections on a recent ‘SU INSIGHTS’ event on the ‘Internal Consultancy’

From ‘right drift’ to ‘left shift’?
Our Head of Policy, Fraser Battye, looks at the challenges facing the intention to shift care ‘from hospital to community’. He suggests that we have missed a critical part of the explanation for why this ‘left shift’ hasn’t taken place following previous initiatives.

Charisma
In this long read, which first appeared in the HSJ, Fraser Battye - our Head of Policy – looks at the role of charisma and innovation in the way that NHS resources are allocated.
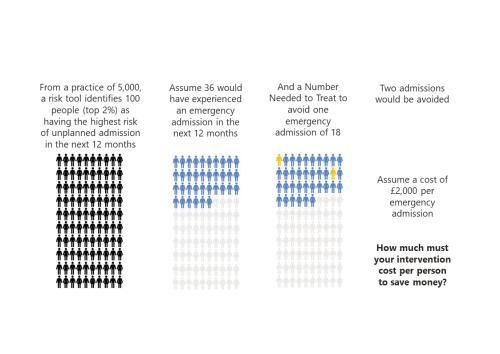
‘To risk stratify or not risk stratify, that is the question’ (At least, it should be)
Risk stratification tools are ubiquitous in healthcare. The concept is simple and seductive.

‘NHS 10 Year Plan’: Strategy Unit consultation response
The Strategy Unit’s response to the Government’s current consultation on the ‘10 Year Health Plan’ for England.

Ara Darzi, Wes Streeting and English health policy. Part 2: cutting the knot
Following on from part one, Fraser continues exploring the Gordian Knot of English health policy.

Ara Darzi, Wes Streeting and English health policy. Part 1: the Gordian Knot
Health policy is not at a crossroads, it is in a bind. Strands so entangled, so complex they resemble a Gordian knot. Can this knot be untied?

The risks of risk stratification
Medical history is full of bizarre and gruesome procedures.

GP services: new analysis and fresh insights
In our latest analysis for the Midlands Decision Support Network (MDSN), we explore the long standing problem of access to GP practice consultations we consider the implications, and explore potential solutions.

Infant feeding problems, lockdown and attendance at Emergency Departments: what’s going on?
From our previous work, with Nuffield Trust and Health Foundation, we know that lockdown had a significant effect on attendance at Emergency Departments (ED). We also know that this effect was very unevenly distributed: some demographic groups stayed away far more than others.

Decisions to admit patients are not solely determined by clinical risk
Whether or not to admit a patient is one of the most routine yet important decisions a doctor in an Emergency Department

Strategy Unit analysis published showing changes in use of emergency departments under lockdown
We know that patterns of access to healthcare have changed during the pandemic.
Health service use in the last two years of life
Health and care services get just one opportunity to support people at the end of their life. When this support is compassionate and appropriate, unnecessary suffering can be avoided and grieving can be eased. When this is not the case, harm and distress can result. The difference in these experiences can be profound.
How will we know if Integrated Care Systems reduce demand for urgent care?
The implications of a blended payment system are far reaching: Decisions about planned activity levels will determine the total funding envelope for urgent care within a system and will influence the behaviour of healthcare providers and the services they deliver to patients.
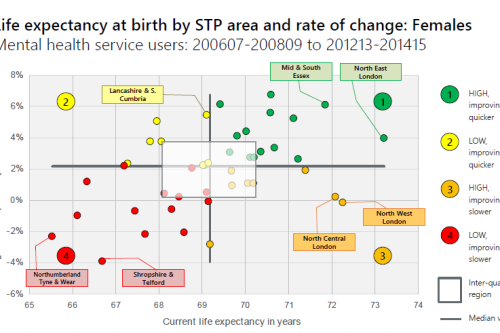
Making the case for integrating physical and mental health services in England - National overview
This is a national overview report of our Making the case for integrating physical and mental health services reporting which took place in July 20
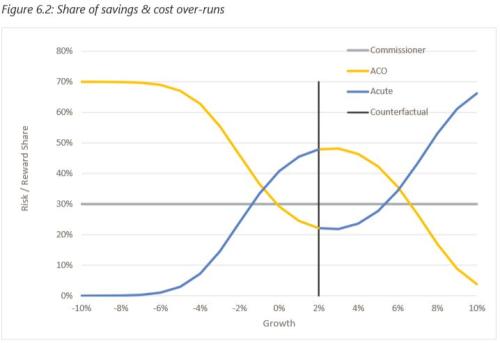
Risk and Reward Sharing for NHS Integrated Care Systems
Risk and reward sharing is a simple and attractive concept, offering a commissioner the opportunity to co-opt and incentivise a provid
Do you like to integrate horizontally or vertically? NHS positions examined
Our latest research paper explores the impact of the different options for integration implemented as a result of the Transforming Community Services policy in 2010. This accompanying commentary reflects on potential implications for the current policy drive towards Integrated Care Systems.